This discussion is now closed.
Check out other Related discussions
- Switching from BA to MSci
- MAT 1996-2006 Solution Thread
- Merton Oxford or St John's Cambridge
- TSR Community Awards 2022: Funniest thread of the year - VOTING CLOSED
- Manchester Medicine Review
- Cambridge Part iii MASt applicants 2021
- Mock MMIs
- University of Sheffield Medicine Student - Ask Me Anything
- Things to do after GCSE as an aspiring medic
- Looking to Speak to Current Medical Students
- Official University of Surrey 2023 Applicant Thread
- STEP 2016 Solutions
- Looking to speak to a vet who qualified as a mature student.
- Bringing horse to uni
- Making Friends
- Career options: Lawyer or doctor
- What is more prestigious?
- Medicine at Leeds, Newcastle or Sheffield?
- tired of school:)))
- Will buying and owning a house affect my student finance?
TSR Med Students' Society Part III
Scroll to see replies
My face when taking blood from a real patient for the first time today.

My face when asked to cannulate an incoming major trauma.

My face when asked to interpret an ECG by a nurse who mistook me for a doctor.

My face when asked to cannulate an incoming major trauma.
My face when asked to interpret an ECG by a nurse who mistook me for a doctor.
(edited 12 years ago)
Original post by Becca-Sarah
It does seem that you can coast through and get a 2.1 but a 1st requires major major effort. The difference between 59.4% and 69.5% is massive.
The thing about research that has pissed me off this week is that even if I had any decent data, I don't have any hope of presenting it anywhere this year as all the abstract deadlines seem to have fallen in January
The thing about research that has pissed me off this week is that even if I had any decent data, I don't have any hope of presenting it anywhere this year as all the abstract deadlines seem to have fallen in January
Same, absolutely agree with the deadlines for abstracts etc. I have the same problem as I have a 6 week time point between patient samples and need both to compare (as they are pre and post radiotherapy). Theres the ISCOMs conference I'm thinking of submitting to (think its this Friday - so if anyone reading it is interested?) and I've only got about 9 patient results. But looked at last years prize winner... and one of their p values was 0.049
 which is incredibly close to accepting null hypothesis. My supervisor won't even let us submit any result like that, hes said only go for something less than 0.01 but if they've gotten a prize... then I'm going to go for it too. (Well maybe not for the more reknowned journals/conferences but for student stuff - will try and submit most results).
which is incredibly close to accepting null hypothesis. My supervisor won't even let us submit any result like that, hes said only go for something less than 0.01 but if they've gotten a prize... then I'm going to go for it too. (Well maybe not for the more reknowned journals/conferences but for student stuff - will try and submit most results).I'm really annoyed now as I didn't want anything lower than a 1st class hons, and I've been working weekends and evenings... but its not my fault if I haven't had any ground breaking results
 I've put the the work in. Gah. Ah well supervisor said I have time to do one more assay so we'll discuss it this Friday with research team, and hopefully he'll accept one of my more exotic ideas... might bring cake for that meeting to sweeten the deal.
I've put the the work in. Gah. Ah well supervisor said I have time to do one more assay so we'll discuss it this Friday with research team, and hopefully he'll accept one of my more exotic ideas... might bring cake for that meeting to sweeten the deal. 
Original post by _Andrew_
How you finding your BSC at leicester? I can't decide whether to stay here and do one next year, or at another medical school
This is going to require a long answer so here goes *deep breath*
Spoiler
Original post by SMed
I did the same for a presentation for journal club. Got a 1st.
Doesn't it scare you that they're professionals and they'll know a lot more about the subject matter? Asking as I've got to do the same thing to a hospital journal club. And well done on the first!

(edited 12 years ago)
Original post by Supermassive_muse_fan
Doesn't it scare you that they're professionals and they'll know a lot more about the subject matter? Asking as I've got to do the same thing to a hospital journal club. And well done on the first!
Well, it was only a 1st for that little assignment.
TBH, I'd been to a few and knew sort of what was expected of me.Right, am I just being majorly derpy or is the hypothalamic-gonadal-pituitary axis just that graph that shows level of FSH/LH/Progesterone/estrogen over time in the menstrual cycle?
Sick, I still haven't got around to ordering my water-cooling bits.
Original post by SMed
It wasn't a real hospital/medics journal club. But it was in front of two other academics who're leading that course module, and then some others from my course.
I finally got a GPU which is due to come just when I start my project, can forget my BSc now.
I finally got a GPU which is due to come just when I start my project, can forget my BSc now.
Sick, I still haven't got around to ordering my water-cooling bits
.(edited 12 years ago)
Original post by RollerBall
Right, am I just being majorly derpy or is the hypothalamic-gonadal-pituitary axis just that graph that shows level of FSH/LH/Progesterone/estrogen over time in the menstrual cycle?
Its not the same graph, you should have negative feedback arrows from gonadal hormones back to hypothalamus and pituitary. Progesterone reduced the frequency (remembered it as progesterone affects pulse) of hypothalamus of secreting GnRH (as its in a pulstile manner and not constant secretion) and oestrogen reduces the amount. Can someone correct me though, did this about a year ago and not 100% sure.
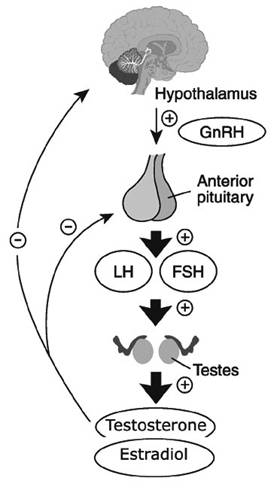
That is what the axis is for males. Its just the whole feedback loop stuff.
The graph you're thinking is just how the hormone levels change over the menstrual cycle but the HPG axis explains why the curves in the cycle are the way they are.
(edited 12 years ago)
Original post by SMed
Well, it was only a 1st for that little assignment. TBH, I'd been to a few and knew sort of what was expected of me.
TBH, I'd been to a few and knew sort of what was expected of me.Any tips

Original post by Supermassive_muse_fan
Its not the same graph, you should have negative feedback arrows from LH/FSH back to hypothalamus and pituitary. Progesterone reduced the frequencey (remembered it as progesterone affects pulse) of hypothalamus of secreting GnRH (as its in a pulstile manner and not constant secretion) and oestrogen reduces the amount. Can someone correct me though, did this about a year ago and not 100% sure.
Ah, yeah, maybe I should have elaborated a little bit. On "my" graph I have that. So I've got the levels of estrogen/GnRH pulsation/progesteron/FSH/LH so it's all covered. As in you can see when estrogen goes up GnRH goes down.
Totally forgot about the male version though, I'll have to recap that.
Original post by RollerBall
Ah, yeah, maybe I should have elaborated a little bit. On "my" graph I have that. So I've got the levels of estrogen/GnRH pulsation/progesteron/FSH/LH so it's all covered. As in you can see when estrogen goes up GnRH goes down.
Totally forgot about the male version though, I'll have to recap that.
Totally forgot about the male version though, I'll have to recap that.
Sorry, can't read. You did mention that but I think I just focused on the 'menstrual cycle' part of the sentence.
All in all it's the same information but different visual representation. So yes.
Original post by Supermassive_muse_fan
Any tips
Basically, you're doing a summary of the paper, along with a brief critical appraisal. The CA can either be after the brief summary, or as you go along each section. It's only 10 minutes, so there's not a lot you can say. For me I found it was just adding a few comments of critique after each summarised section. Then just some general comments at the end with how the study fits into what we know already and the current research that's out there. Is the study relevant and applicable to something useful for us (the audience you're speaking to or clinicians in general). Read around the topic a bit, and have a think about the limitations. If there are any specific techniques or anything that are mentioned in the study, have a read about them, especially if they're well known. A friend got marked down from a 1st to a high 2.1 because he couldn't remember what a PET scan was.
Original post by Supermassive_muse_fan
This is going to require a long answer so here goes *deep breath*
This is going to require a long answer so here goes *deep breath*
Spoiler
Thank you- that has been incredibly useful! Any tips for semester 4, it seems so much more relaxed than last semester
!If i watch another cholectomy im going to crack. Emergency surgery in a small dgh is a complete joke!!
Original post by _Andrew_
Thank you- that has been incredibly useful! Any tips for semester 4, it seems so much more relaxed than last semester!
!Enjoy it whilst you still can! But seriously,semester 3 is super crammed and then you spend semester 5 stressing out about Phase 1. I'd actually just try and finish the dissertation because as soon as its over it feels like you've got your life back
. (She says in a jokily manner but its very much true). But yes sort of relax a bit and ooh how are you finding CPC?What SSC are you doing? And do not pick 'brain disorders and cell signalling' for semester 5. I did that thinking it would help immensely with neuro and M&R. It didn't and just added to the work.
Original post by SMed
Spoiler
Merci beaucoup! Very helpful

(edited 12 years ago)
Original post by Supermassive_muse_fan
that axis is going to be insufficient to explain the female reproductive cycle, it ignore the roles of other hormones eg the inhibins, activins etc but it'd take forever to type out why so i won't
. the gondatrophin axis in the laydeez is more complex than the standard HPA/HPT etc because superimposed on the circadian rhythm is the infradian aspect.Original post by John Locke
that axis is going to be insufficient to explain the female reproductive cycle, it ignore the roles of other hormones eg the inhibins, activins etc but it'd take forever to type out why so i won't . the gondatrophin axis in the laydeez is more complex than the standard HPA/HPT etc because superimposed on the circadian rhythm is the infradian aspect.
. the gondatrophin axis in the laydeez is more complex than the standard HPA/HPT etc because superimposed on the circadian rhythm is the infradian aspect.That was just the first one that google gave me and I wanted to portray the feedback loop as the axis.
Actually you know the biological clock is meant to be 25 hours long? They did that in sleep physiology with some patients, and concealed when it was day and night and found all the patients went into a 25 hour day cycle.
Might explain why I'm always behind on work...
Original post by Supermassive_muse_fan
That was just the first one that google gave me and I wanted to portray the feedback loop as the axis.
Actually you know the biological clock is meant to be 25 hours long? They did that in sleep physiology with some patients, and concealed when it was day and night and found all the patients went into a 25 hour day cycle.
Might explain why I'm always behind on work...
Actually you know the biological clock is meant to be 25 hours long? They did that in sleep physiology with some patients, and concealed when it was day and night and found all the patients went into a 25 hour day cycle.
Might explain why I'm always behind on work...
In young adults, 20-50, the clock runs long, around 24.5 hours - so that means we naturally want to get up half an hour later each day. There are studies showing a class of photoreceptors in the retina that detects light independently of the rods and cones and this acts as a reset for the clock depending on light - for some it is dawn, for others, dusk.
Do you mean the aschoff experiments when they locked the students into dungeons? That was great for the guy that had a uber long clock, not so good for the chap running on half time.
I did a course on clocks, sleep and biological time - best course ever
Original post by crazylemon
I was in theatre with one of amateur transplants today
Which one?
Original post by Talexe
Which one?
Since one of them quit medicine to do full time comedy, I'd put good money on it being Suman.
Original post by crazylemon
I was in theatre with one of amateur transplants today
Original post by Talexe
Which one?
What's this about TED talks at Imperial? Is it real TED or what?
Sees pre-clinical post.....
Does not read
Does not read
Related discussions
- Switching from BA to MSci
- MAT 1996-2006 Solution Thread
- Merton Oxford or St John's Cambridge
- TSR Community Awards 2022: Funniest thread of the year - VOTING CLOSED
- Manchester Medicine Review
- Cambridge Part iii MASt applicants 2021
- Mock MMIs
- University of Sheffield Medicine Student - Ask Me Anything
- Things to do after GCSE as an aspiring medic
- Looking to Speak to Current Medical Students
- Official University of Surrey 2023 Applicant Thread
- STEP 2016 Solutions
- Looking to speak to a vet who qualified as a mature student.
- Bringing horse to uni
- Making Friends
- Career options: Lawyer or doctor
- What is more prestigious?
- Medicine at Leeds, Newcastle or Sheffield?
- tired of school:)))
- Will buying and owning a house affect my student finance?
Latest
Trending
Last reply 6 hours ago
Public Health ST1 Programme 2024 Entry ThreadLast reply 6 days ago
Has anyone left medical school? What are you doing now?Last reply 2 weeks ago
Doing an observership in the US during F1?Last reply 3 weeks ago
University: Failed OSCE/Module. Thoughts on appeal?Last reply 2 months ago
FY1 & FY2 for international medics graduating in 2024Last reply 2 months ago
Question about training to be a Public Health Consultant.Trending
Last reply 6 hours ago
Public Health ST1 Programme 2024 Entry ThreadLast reply 6 days ago
Has anyone left medical school? What are you doing now?Last reply 2 weeks ago
Doing an observership in the US during F1?Last reply 3 weeks ago
University: Failed OSCE/Module. Thoughts on appeal?Last reply 2 months ago
FY1 & FY2 for international medics graduating in 2024Last reply 2 months ago
Question about training to be a Public Health Consultant.

