This discussion is now closed.
Check out other Related discussions
- Skin help
- Effects of Citalopram (20mg) on me, and general situation?
- Does anyone have any experience of propranolol?
- Help with skin care
- Eligibility/ entitlement to Council housing
- How bad is it to take 30-50mg of codeine a day
- question ... can anyone help please?
- d d d d dd d d
- does anyone know what the combined pill does?
- How long does it take for iron to be absorbed?
- how do you do this please explain steps
- Are there any antidepressants that don't cause nausea/sickness
- Preferred College
- Acne /skin texture on the face
- Living with cat allergies?
- Abnormal liver function test results, is there any hope things will get better?
- Physics Alevel question :- electromagnetism induction and alternating current
- quinoderm acne cream?
- Norethisterone - Do the benefits outweigh the side effects?
- HELP: Submitted wrong coursework on Turnitin on an MCF extended deadline
Q./ A person suffering liver damage is often prescribed smaller doses ...
ok
(edited 12 years ago)
I'm guessing the first question is something to do with the Liver being responsible for modifying Xenobiotics for degredation and removal from the body. Therefore a drug dose that would say be made ineffective after a day in someone with no liver damage, may last two days in someone with liver damage.
ark1987
Q./ Jaundice is frequently and indication of liver damage. IN this condition, the skin takes on and abnormal yellow colouration because bile pigments are circulating in the blood.
Explain why bile pigments are circulating in the blood in a person suffering from jaundice. ?
Explain why bile pigments are circulating in the blood in a person suffering from jaundice. ?
Haemoglobin is eventually broken down to bilirubin
Bilirubin (a yellow pigment) is excreted in bile salts and eventually got rid of in the body in the faeces
So if you have bile salt circulating, bilirubin is not excreted and so you get yellow pigmented skin - jaundice.
Why this happens, I dunno.
ark1987
Q./ Jaundice is frequently and indication of liver damage. IN this condition, the skin takes on and abnormal yellow colouration because bile pigments are circulating in the blood.
Explain why bile pigments are circulating in the blood in a person suffering from jaundice. ?
Explain why bile pigments are circulating in the blood in a person suffering from jaundice. ?
Jaundice is yellowing of the skin, sclera (the white of the eyes) and mucous membranes caused by increased levels of bilirubin in the human body. Usually the concentration of bilirubin in the blood must exceed 2–3mg/dL for the coloration to be easily visible.
Bilirubin (bile pigment) will be circulating in the bloodstream for one of 3 reasons:
Pre-hepatic jaundice - where the haemoglobin in blood is broken down (haemolysis) in increased amounts, so bilirubin there is more bilirubin which needs to be excreted. Certain genetic diseases, such as glucose 6-phosphate dehydrogenase deficiency, sickle-cell disease and thallassaemia can lead to increase red cell lysis and therefore haemolytic jaundice. A less common cause is Gilberts syndrome (which causes enzymatic abnormalities).
Intra-hepatic - This is where the hepatocytes (liver cells) are damaged and so are unable to excrete bilirubin into the gallbladder and cystic duct. This is usually due to: viruses (hep A, B, C and Epstein-Barr); drugs (paracetemol overdose, statins, MAOIs, etc); alcoholic hepatitis; cirrhosis; cancer metastases; haemochromatosis; Wilson's disease (copper deposition)
Post-hepatic - this is where there is a blockage in the flow of bile out of the gallbladder, causing a backlog, causing bilirubin to be excreted into the bloodstream. As this bilirubin has been processed by the liver it is conjugated (as opposed to unconjugated as in most cases of pre- and intra- hepatic jaundice) - this allows it to be excreted in the urine (so it becomes darker) and the faeces become pale and greasey (due to no pigment from bilirubin, and greasy due to lack of fat emulsification by bile, therefore it isn't taken up, so the faeces become fatty - steatorrhoea). The obstruction may be luminal (blockage within bile duct – commonly gallstones), mural (defect within bile duct wall – due to benign post-op stricture, or malignant tumour), or extra-luminal (pressing on the bile duct – e.g. due to pancreatic carcinoma or lymphadenopathy). A rare cause of obstructive jaundice is Mirizzi's syndrome (where a gallstone becomes ipacted in the wall of the cystic duct leading out of the gallbladder).
The breakdown of haemoglobin:
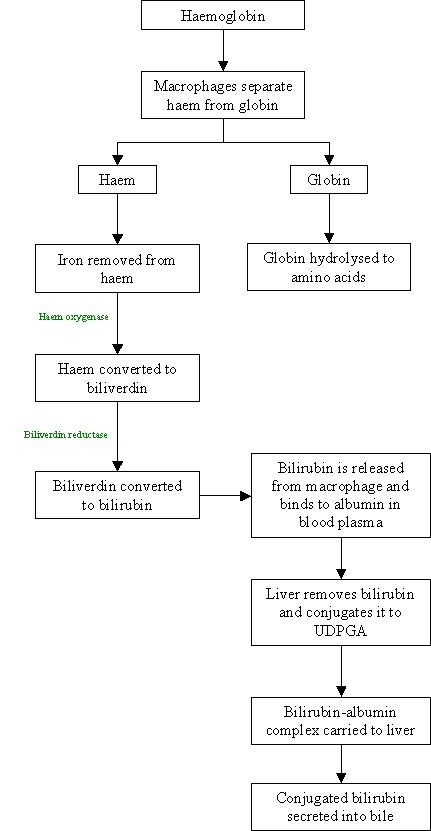
/edit: sorry, the second and third to last steps are the wrong way round
Related discussions
- Skin help
- Effects of Citalopram (20mg) on me, and general situation?
- Does anyone have any experience of propranolol?
- Help with skin care
- Eligibility/ entitlement to Council housing
- How bad is it to take 30-50mg of codeine a day
- question ... can anyone help please?
- d d d d dd d d
- does anyone know what the combined pill does?
- How long does it take for iron to be absorbed?
- how do you do this please explain steps
- Are there any antidepressants that don't cause nausea/sickness
- Preferred College
- Acne /skin texture on the face
- Living with cat allergies?
- Abnormal liver function test results, is there any hope things will get better?
- Physics Alevel question :- electromagnetism induction and alternating current
- quinoderm acne cream?
- Norethisterone - Do the benefits outweigh the side effects?
- HELP: Submitted wrong coursework on Turnitin on an MCF extended deadline
Latest
Trending
Last reply 2 days ago
GCSE Biology Study Group 2023-2024Last reply 5 days ago
A-level Biology Study Group 2023-2024Last reply 1 week ago
Need detailed and specific OCR Biology notes before alevel exam.Last reply 1 week ago
SNAB biology- Access to end-of-topic tests/summaries 2024Last reply 1 week ago
a level biology mitosis questionLast reply 2 weeks ago
Biology surface area to volume rationLast reply 3 weeks ago
aqa biology aslevel calculation question FVCPosted 1 month ago
SNAB biology 2024 scientific articleLast reply 1 month ago
Resources for edexcel a (snab) a level biology?Last reply 1 month ago
Im losing my mind over this and I don't know where I keep going wrongLast reply 1 month ago
Aqa biology a level paper 3 2023Last reply 2 months ago
AQA A Level Biology Paper 1 2018Last reply 3 months ago
how do you do this please explain stepsLast reply 5 months ago
biology math question ratios alevel aqaLast reply 5 months ago
biology aqa alevel proteins question past paperTrending
Last reply 2 days ago
GCSE Biology Study Group 2023-2024Last reply 5 days ago
A-level Biology Study Group 2023-2024Last reply 1 week ago
Need detailed and specific OCR Biology notes before alevel exam.Last reply 1 week ago
SNAB biology- Access to end-of-topic tests/summaries 2024Last reply 1 week ago
a level biology mitosis questionLast reply 2 weeks ago
Biology surface area to volume rationLast reply 3 weeks ago
aqa biology aslevel calculation question FVCPosted 1 month ago
SNAB biology 2024 scientific articleLast reply 1 month ago
Resources for edexcel a (snab) a level biology?Last reply 1 month ago
Im losing my mind over this and I don't know where I keep going wrongLast reply 1 month ago
Aqa biology a level paper 3 2023Last reply 2 months ago
AQA A Level Biology Paper 1 2018Last reply 3 months ago
how do you do this please explain stepsLast reply 5 months ago
biology math question ratios alevel aqaLast reply 5 months ago
biology aqa alevel proteins question past paper


